

The scattergun approach in research - a deep dive into CDK4/6 inhibitors tested in the neoadjuvant setting.
About forty trials enrolling thousands of patients have been launched since 2010.

In the past decade, an area of research that has attracted much interest from scientists has been the development of CDK4/6 inhibitors (CDK4/6i) for neoadjuvant HR-positive, HER2-negative early breast cancer. Six years ago, in 2018, 16 trials were registered on ClinicalTrials.gov in this setting, involving a total of 2,290 patients. If you look now, there are about forty trials with thousands more patients to explore the potentials of these therapies (see at the end of the post or here).

Most of these trials are independent investigator-initiated studies that are exploratory and underpowered. They often use the downstaging of Ki67 antigen (a marker for tumour cell growth), as a primary endpoint. While CDK4/6i can reduce Ki67 expression during treatment, the clinical impact of it remains unknown. What we do know is that there can eventually be a rebound in Ki67expression when the treatment is stopped, as was seen in NeoPalAna and NeoMONARCH. Examining a small series of matched tumour biopsies before and after CDK4/6i treatment showed that three out of seven cases had evolved to a triple-negative profile. The neoadjuvant FELINE trial also demonstrated that CDK4/6i accelerated the phenotypic switch from luminal-like to basal-like, led to the loss of estrogen signalling and increased resistance to endocrine therapy.
The overall results so far show that pathologic response rates or pathological complete response (pCR) rates remain low, and there appears to be no impact on invasive disease-free survival (iDFS) either. However, we cannot be certain because underpowered trials with limited follow-up may not reveal the differences.
Current approach to research may damage trust in clinical trials
Despite numerous trials involving thousands of patients, there is still no evidence that neoadjuvant CDK4/6 inhibitors can improve survival or replace chemotherapy. Instead, we continue to see similar or slightly different trials being rolled out in the same setting. Some of these trials try to find alternative outcome measures, while others modify treatment durations or explore new combinations. Yet, this scattergun approach to research seems to be getting us nowhere and is failing to provide meaningful benefits for patients and society.
Here are some thoughts on these trials:
1. Non-effective neoadjuvant therapies could increase the risks of developing unresectable tumours and metastasis. Why, then, do we plan studies involving 8-9 months of neoadjuvant therapy and delays in surgery?
2. Why conduct an early phase trial in the neoadjuvant setting when our goal is to cure? We should avoid burdening patients with the long-term side effects of uncertain regimens. For instance, adding abemaciclib and durvalumab to endocrine therapy may raise concerns, since neither has demonstrated a clinical advantage in early setting, and the long-term safety and tolerability of the combination is unknown (fortunately the study is now withdrawn). As one might expect, adding nivolumab and palbociclib to endocrine therapy resulted in significant toxicity and treatment discontinuation, which eventually led to early closure of the CheckMate 7A8 study.
3. Why giving CDK4/6i in both the neoadjuvant and adjuvant settings, when the benefits of the neoadjuvant use still need further investigation and overall survival impact in the adjuvant setting is uncertain and needs further follow-up? See also the recent ODAC recommendations. In ROBOLARIS, it is particularly puzzling that adjuvant ribociclib is planned to be given to those who did not respond to this compound in the neoadjuvant setting.
What would be the best approach?
While it may be impossible to define a "best" approach, here are some general thoughts.
Perhaps one reason we see many of the same trials is the lack of transparency in studies, including the incomplete analysis and publication of clinical data and exploratory biomarker studies. More transparency can help patients make better-informed decisions when participating in trials. Patient advocacy groups should scrutinise study designs and publications to enhance trial quality and patient safety.
More collaboration between research groups can enable the design of studies with sufficient power, relevant clinical endpoints and adequate follow-up.
Additionally, better orchestration is needed between investigator-initiated trials. Since pharmaceutical companies typically provide trial medication and/or study budgets, they have a responsibility to help coordinate these trials effectively.
Finally, a thorough analysis of all existing studies combined with better patient follow-up, can provide clearer insights into the efficacy and safety of these products and guide future research.
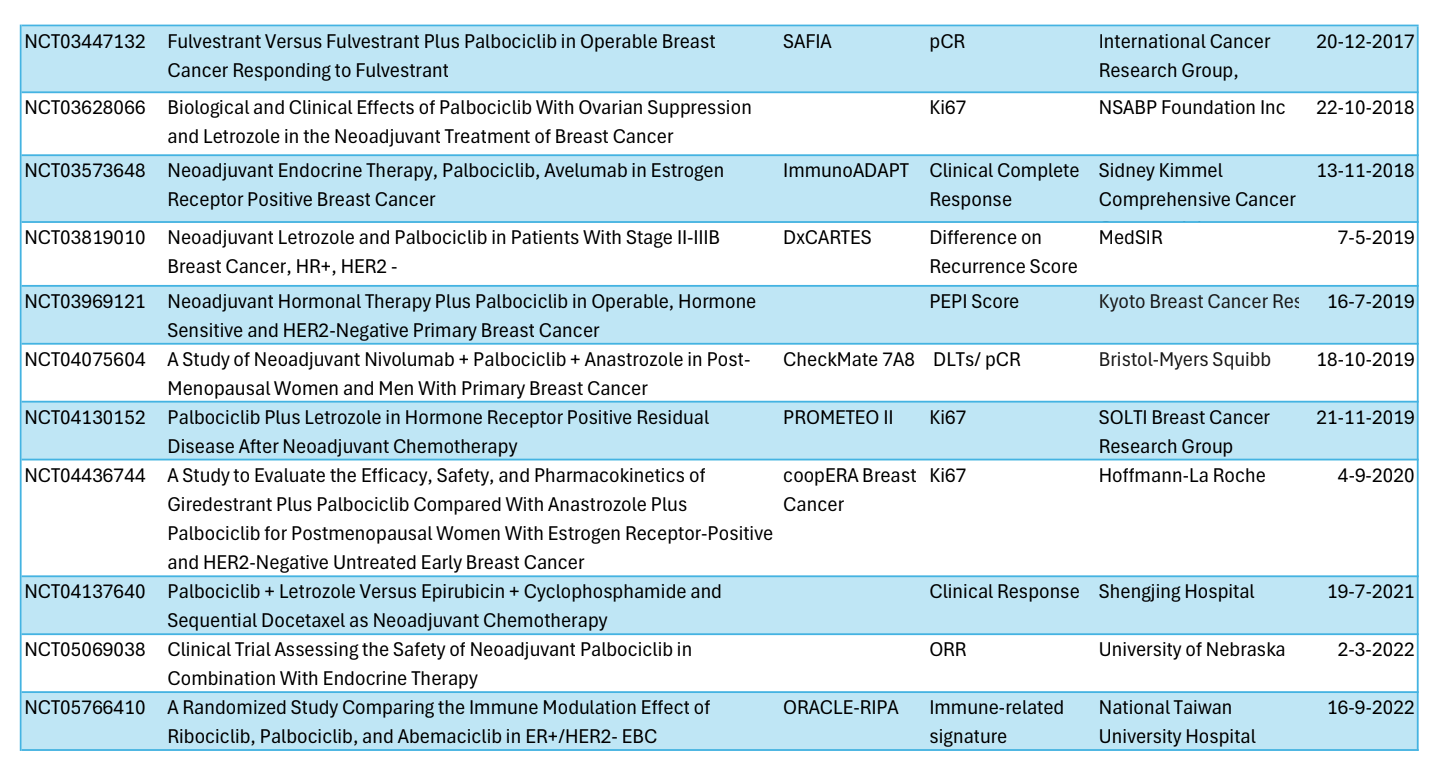
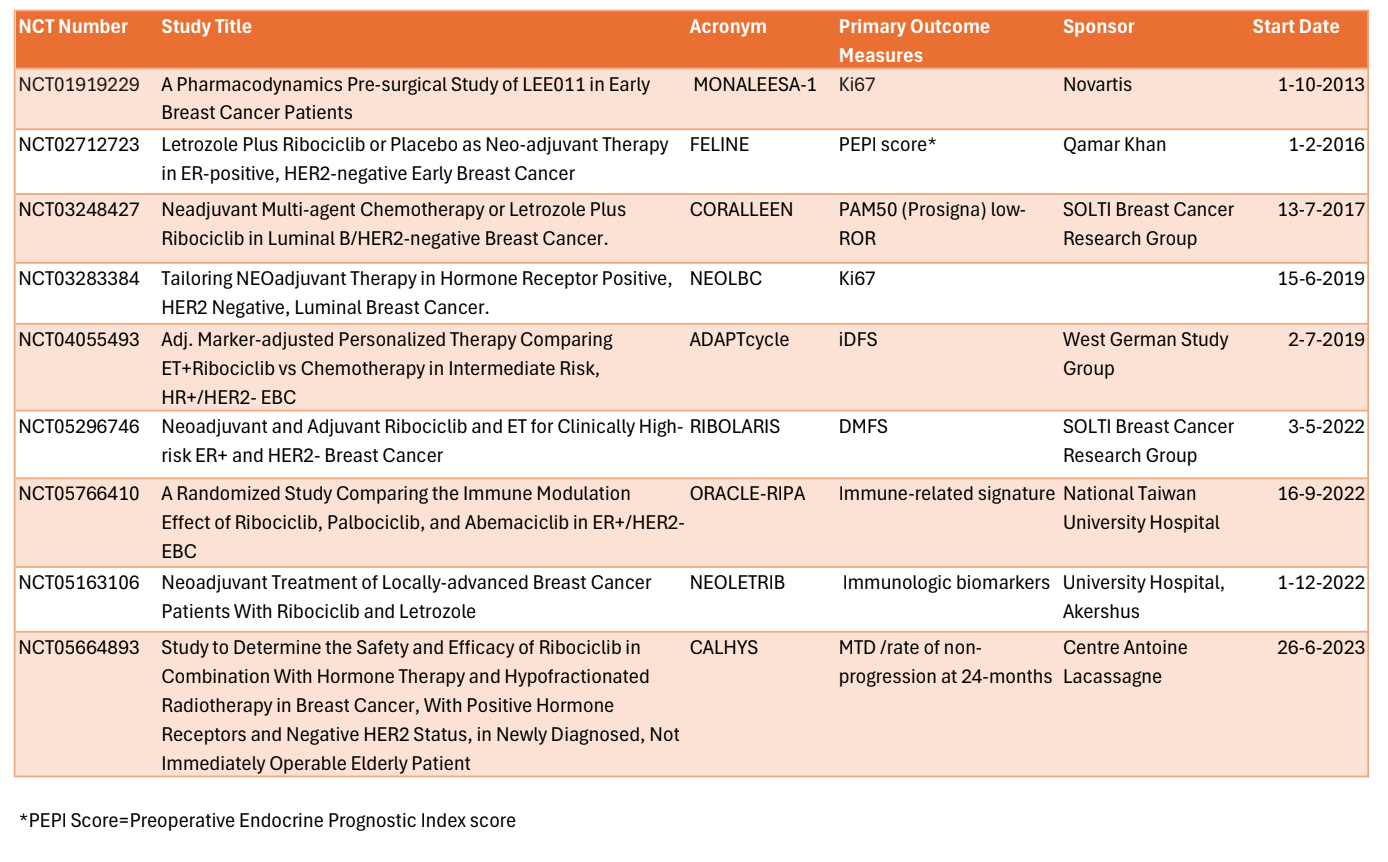
Below are the forty trials that have been launched (palbociclib in blue, abemaciclib in green and ribociclib in orange, also available here).


 | A guest post by
|