



NEW JAMA PAPER - MRD+ in AML prior to transplant does poorly. Stronger conditioning helps the young - Wait, Not So Fast
Obvious and dangerous conclusions

There's a new paper out in JAMA that sequences a lot of people undergoing transplant for AML. Let's give them credit for hard work. Now, let's interrogate the claims.
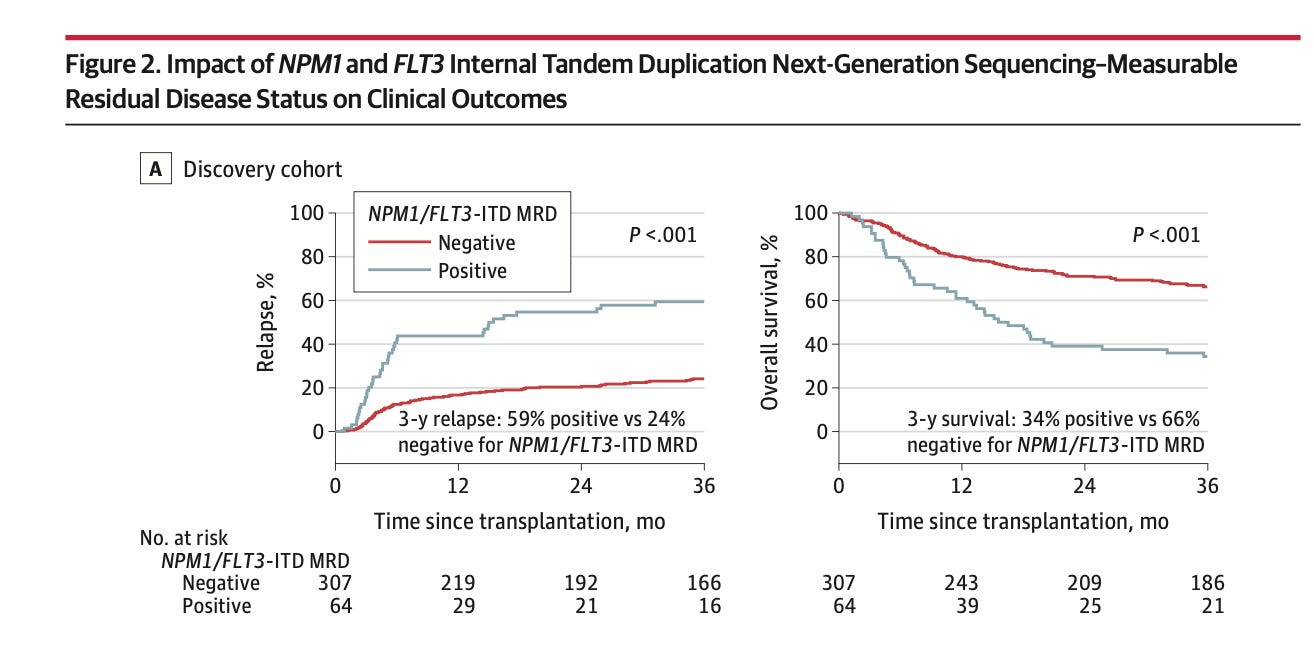
First the authors show that it's better to have less cancer than more cancer when you get a transplant.
The results apply just to people withNPM1, FLT3,, IDH1 or IDH2, and/or KIT. If you don’t have one of these, you are excluded. More vs less cancer is based on a blood sample (median ~9 days) prior to transplant, and an MRD analysis. Honestly, the result is unsurprising because a 2021 paper shows basically the same thing.

Mary Elizabeth Percival found the same thing in 2021. I don’t see this paper as cited in the JAMA paper, yet the central finding is the same (it uses flow)


The Percival paper goes further and stratifies by CR and CR with incomplete hematologic recovery which does worse— also unsurprising.
The current paper reaches similar conclusions.
Both papers find the rate of MRD + is about the same. The JAMA paper 17.3% had detectable MRD— the Percival paper— 18% and 12% (CRi and CR respectively).
Having said that, there is a big limit to the JAMA paper. Authors don't adjust for *all* covariates that can predict the outcome.
You need to show that MRD positivity is independently associated with bad outcomes adjusting for all of the variables you ALREADY HAVE at baseline.
But one variable that the current paper is not adjusting for is the precise blast percentage on pre-transplant marrow. CIBMTR is proving the assurance that these patients are in CR, but the Percival paper says that is defined only as <5% blasts, “CR with fewer than 5% marrow blasts is an inadequate assessment of disease status and that both count recovery and MRD status also need to be considered.”
So a person with 5% blasts is getting MRD testing? Why do I need to run a blood test— I know they have 5% blasts? (I concede that we don’t know if these are cancer vs normal hematopoesis, but it should still be adjusted for).
The exact percentage of blasts should be included as a variable to show what added benefit a blood MRD tests adds beyond the path report. My best guess is CIBMTR does not collect this data (I’ve emailed to find out). But the paper doesn’t say it adjusted for it.
Since they do not adjust for this, we don't know if we're learning anything beyond the pre-transplant marrow.
Let me put it another way. If there are 0% blasts, ok it makes sense to send your blood test (maybe), but if there are 5% blasts. I strongly suspect they have residual disease. And what if they have 6% or 10% but CIBMTR has miscoded it. In all these cases, why do I need to send a blood test? The paper should adjust for this.
Second, then the authors get out over their skis. They compare reduced intensity versus myeloablative transplant. They also compare melphalan versus other regimens for reduced intensity. This is the problem.
These choices are not randomly made. And this is not a randomized trial. The authors write

But of course, doctors are going to offer myelo-ablative regimens to healthier young people, and the poor young person who you take to RIC is going to be sicker. These outcomes must be validated prospectively in randomized fashion before we conclude that this prognostic marker can be overcome by therapeutic intensity.
Also, if I am reading eFigure11 right, it shows this doesn’t hold up in multivariable analysis. Am I missing something?

Ultimately, for these reasons, the authors fail to persuade us that this should be part of universal testing.
After reading the paper we are left with:
Don't know if you're offering prognostic value beyond the blast % in marrow pretransplant
You have not proven that acting upon these variables differently improves outcomes— yet as I will show below, the PI says it is ready for prime time.
Your observational results are salami sliced by age, intensity of preparatory regimen, and specific drugs used. (wobbly result)
Why did they not break it out by CR vs CRi, which is already known to be prognostic (Percival)?
I compliment the investigators for working hard. But the PI’s comments on social media are not appropriate. It is premature to pay for this routinely; The authors have not proven that routine application of the test improves outcomes. Also the test will be used on ~500 people per year— by their own numbers. How much will it cost to generate ROI?


How do you get 500 per year? It is right there

Turns out that is just 16% of people undergoing allo for AML

If you like this analysis share & subscribe
Vinay, could you please explain your point about bone marrow blast percentage before allo? You seem to be making the argument that 4.9% is worse than 2.7% which is worse than 1.1% which is worse than 0%. But isn't it also the case that a healthy individual with no leukemia or MDS may have up to 5% blasts in their bone marrow? Nevertheless, you're saying that higher blast percentage (even below 5%) is a negative prognostic indicator for patients about to undergo allo, is that right? Could you please provide a reference? Thanks, and great post!