



Immune Checkpoint Inhibitors: 10-Year Results in Melanoma Are Now Out – Let's Reflect on These Impressive Advances.
Remarkable advances and remaining questions.

The 10-year results of first-line immune checkpoint inhibitors in melanoma are truly remarkable. They have just been published in the New England Journal of Medicine (also accessible here).

In short, in a condition where survival was historically limited to just a few months in most cases — metastatic melanoma — we now see treatment groups with around 40% of patients still alive after 10 years, meaning many can now be considered cured.
This is shown in the survival curves below: 43% of patients in the IPI-NIVO-first arm (combination of ipilimumab and nivolumab) and 37% of patients in the NIVO-first arm (nivolumab alone) are alive at 10 years.
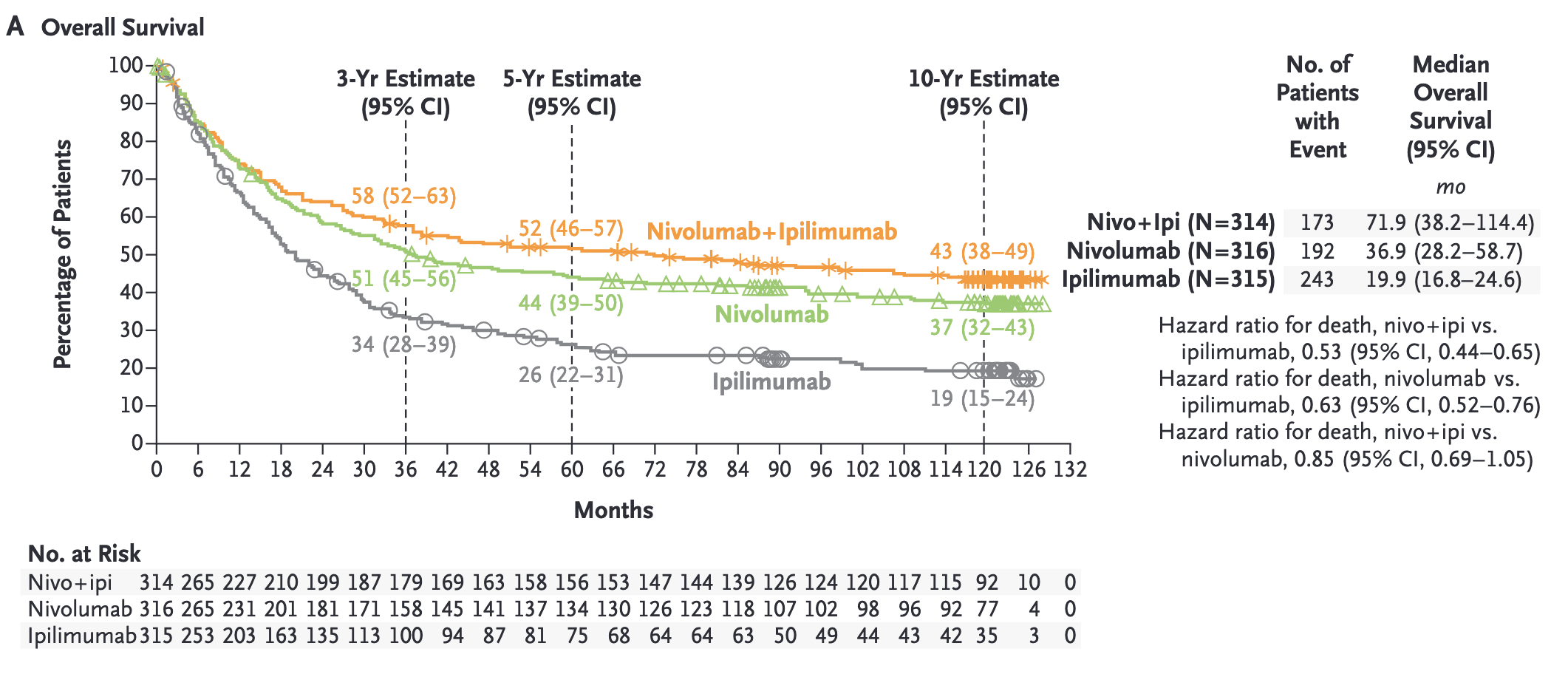
IPI-NIVO (orange curve) appears to be superior to NIVO (green curve). Is this conclusion valid?
This question is important because IPI-NIVO results in 63% grade 3-4 toxicities. These toxicities can lead to weeks or months of corticosteroid use and debilitating conditions, likely affecting patients’ quality-of-life. In contrast, NIVO’s long-term toxicity data show 25% grade 3-4 toxicities. While not trivial, this is 38 percentage points lower than IPI-NIVO.
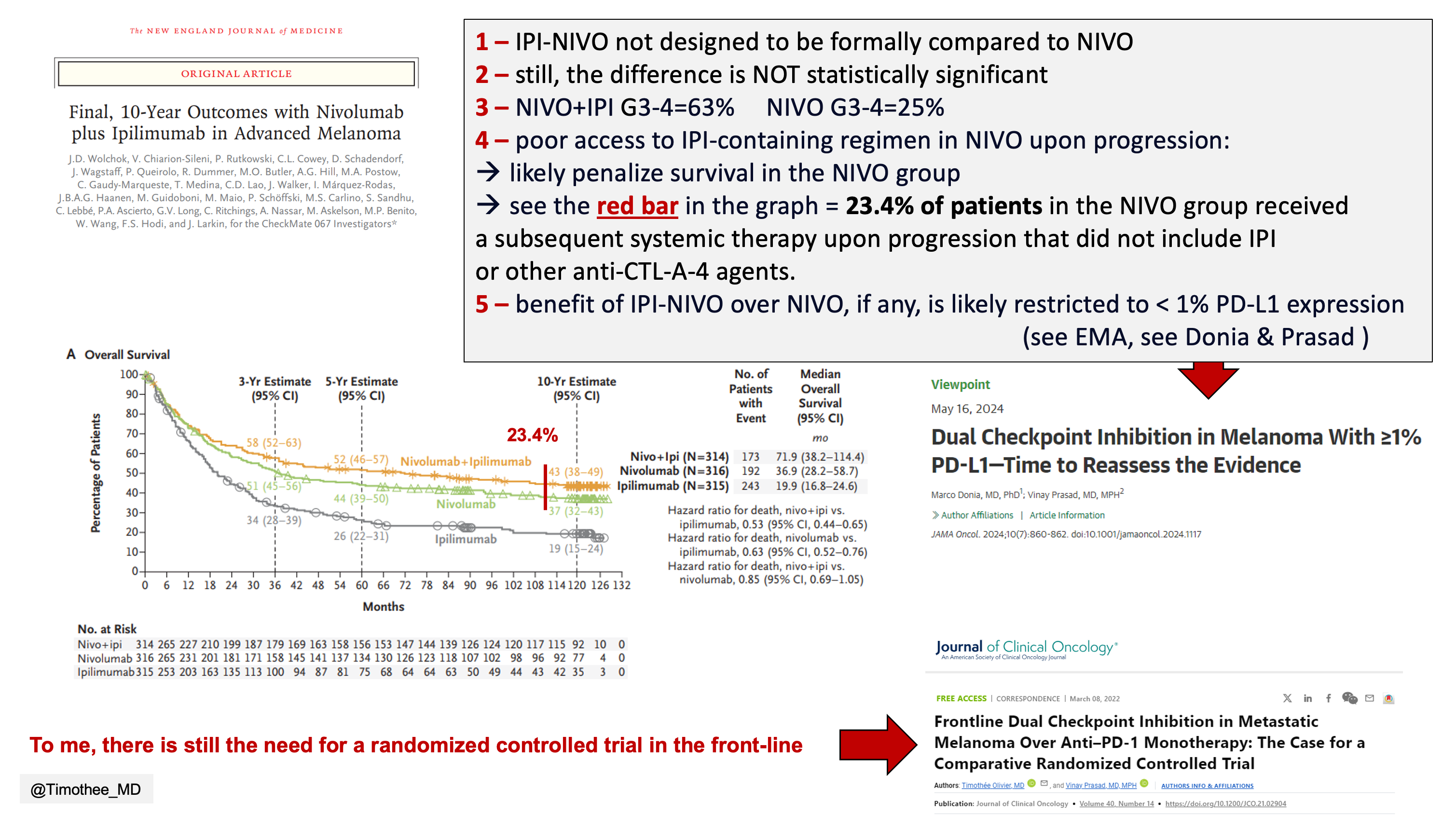
Three points can be made against concluding the superiority of IPI-NIVO over NIVO:
IPI-NIVO was not designed to be formally compared to NIVO.
The difference is not statistically significant.
Poor post-progression care: 23.4% of patients in the NIVO group received a subsequent systemic therapy upon progression that did not include IPI (or other anti-CTL-A-4 agents). If even a fraction of these patients had derived the long-term benefit expected from an IPI-containing regimen upon progression, the difference seen between the curves could have disappeared (see the red bar below, which is significantly wider than the difference between the orange and green curves).

The benefit of first-line IPI-NIVO, if any, is likely restricted to < 1% PD-L1 expression
In melanoma, there is mounting evidence suggesting that first-line IPI-NIVO does not add clinical efficacy over other strategies in patients with ≥1% PD-L1 expression, which constitutes 40% of them.
Check out the work published by Marco Donia and Vinay Prasad in JAMA Oncology (full link here). It’s also covered in the drugdevletter (link here).
Conclusion
In short, the observed results represent an immense gain for patients and are probably one of the biggest advances seen in oncology in recent decades. However, the combination of IPI-NIVO is much more toxic than NIVO alone, and its formal superiority has yet to be demonstrated. I still believe there is a need for a randomized trial in this area, as we previously outlined with Vinay Prasad in the Journal of Clinical Oncology. Here is a one slide summary.
Spot on! Costs an issue as well...
This paper illustrates the old dictum, “More drugs does not necessarily mean better results.”