



Eli Lilly's Court Victory: Dutch Agency Must Reevaluate Abemaciclib Amid Controversy
Eli Lilly’s court appeal to override the negative assessment of abemaciclib in the Netherlands

I want to introduce this article by Sahar van Waalwijk from the Netherlands. Recently, Eli Lilly, apparently vying to appear as a the villian in a movie, sued the Netherlands for not paying for a costly, uncertain cancer drug. Lilly won! This is a damaging precent in Western Europe, and Sahar explains the case. Remember to support content like this consider subscribing
Vinay Prasad MD MPH
Eli Lilly's Court Victory: Dutch Agency Must Reevaluate Abemaciclib Amid Controversy
Recently, in an unprecedented move, the pharmaceutical company Eli Lilly has taken a national Health Technology Assessment (HTA) body to court to override their negative assessment.

The reason is that Eli Lilly has made significant investments in developing abemaciclib and a negative reimbursement decision leads to substantial financial losses.
The global open-label phase III trial, monarchE (Johnston et al., 2023; Rastogi et al., 2024), has indeed been a significant investment for the company. Originally, the trial planned to randomise 3580 high-risk, node-positive HR+ HER2- breast cancer patients, between 2 years of abemaciclib combined with standard adjuvant endocrine therapy (ET) versus standard adjuvant ET. Later, through an amendment, the sample size was increased by 1000 patients, but eventually ended up over-randomising 2057 patients, bringing the total to 5637.
Overpowered trials have the potential to identify differences that are statistically significant but not clinically meaningful. In November 2023, this indication received a negative recommendation from the Dutch Society for Medical Oncology (NVMO) because it did not meet their defined threshold for ‘minimal important difference’ (based on PASKWIL-2023 criteria, used for drug evaluation in the Netherlands, updated in 2023).
In the following month, the national HTA body in the Netherlands – the Healthcare National Institute – also published its negative assessment and advised the Dutch government against including this indication in the national insurance package.
Five months later, Lilly took the HTA body to court.
The Case
Eli Lilly’s claim was that the adjuvant indication of abemaciclib meets the state-of-the-art criterion required for reimbursement in the Netherlands, and sought the court to instruct the HTA body to disregard the current pharmacotherapeutic evaluation and proceed with the next steps in the procedure, which include budget impact analysis and pharmacoeconomic evaluation. Here is the judge’s ruling (you can use an online browser translator).

Alternative reliefs included that the HTA body should retract the current report and reassess the indication based on the surrogate endpoint of disease-free survival (DFS) instead of Overall Survival (OS). This reassessment should use either the older version of the assessment criteria of the Dutch Medical Society for Oncology (PASKWIL-2018), which are less strict than the current ones (PASKWIL-2023), or follow international guidelines and ESMO-Magnitude of Clinical Benefit Scale, which attributed the highest score in the adjuvant setting to abemaciclib in this indication – an A Score.
During the Case, the parties agreed that the essence of these preliminary relief proceedings was whether the assessment had been correctly carried out. Lilly claimed that the state-of-the-art criterion should be considered from an international perspective, arguing that the indication is reimbursed in many European and North American countries and is recommended in various international guidelines, including ESMO. In contrast, the HTA assessment focuses solely on the local recommendations of Dutch oncologists. They also claimed that the stricter evaluation criteria of PASKWIL-2023, which have been enforced since last year, are not supported by all oncologists and are rejected by patient advocacy group for breast cancer.
Subsequently, the Healthcare Institute counterargued that due to their public duty, their recommendations should be based on the most recently accepted standards of the relevant medical society (in this case PASKWIL-2023). Besides, each country has its own reimbursement system and methods of assessment and that these are not harmonised at the European or international level. The mere fact that a medicine is reimbursed in another country does not mean that it meets the criteria in the Netherlands and must be covered.
The court held, however, that the HTA body, based on its own framework, should consider the international perspective. Given that sister organisations in almost all European countries, the US, and Canada have given positive assessments, it is puzzling why the HTA report does not mention this and clarify why it holds a different opinion.
Overall Survival: mature or not?
A major objection of Eli Lilly was that the HTA had considered only OS as a crucial outcome, despite the data not being mature. The HTA report had concluded that the OS data were 'mature enough’ to draw conclusions. Their analysis was supported by the report of an external statistician and subsequently confirmed by an independent committee of experts. The court agreed with Eli Lilly that it is puzzling that the Dutch HTA body is making predictions regarding OS, especially when the international scientific community suggests that the available data are currently immature.
Court orders reassessment
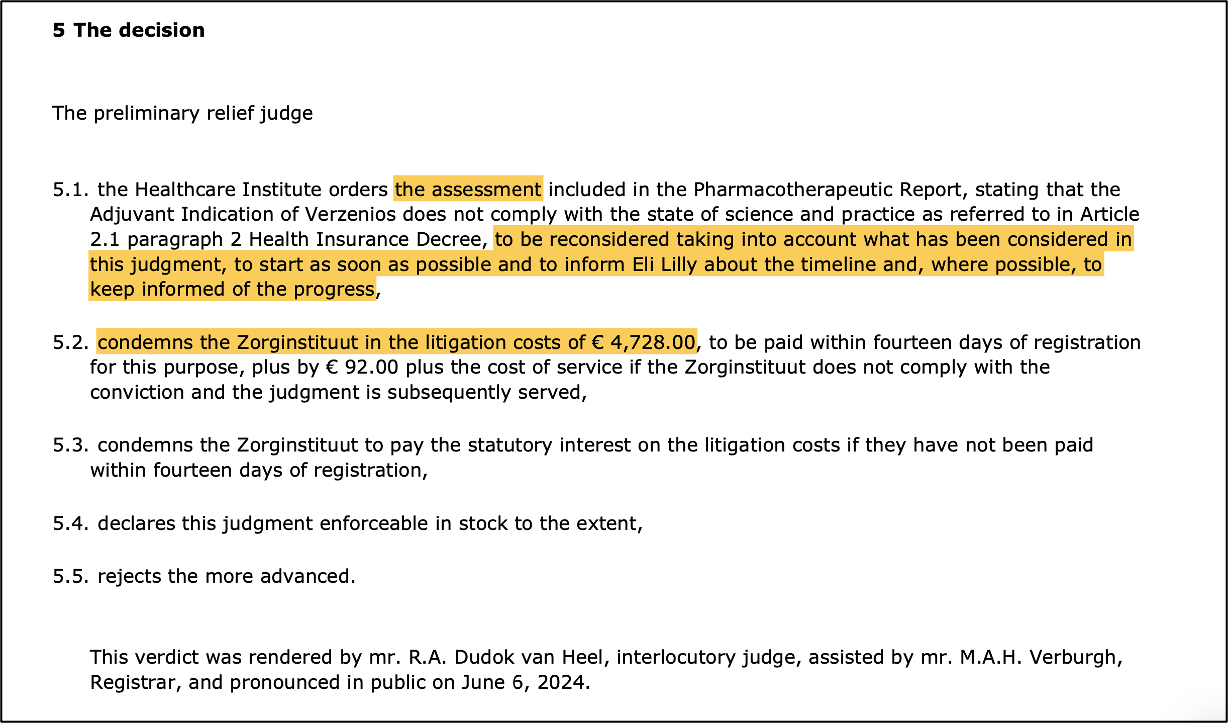
The court ruled that the pharmacotherapeutic report, and therefore the negative assessment, was flawed and that the HTA body had acted unlawfully towards Lilly. The motivations of the HTA report were inadequate; it should have explained why additional statistical analyses were carried out instead of solely relying on published peer-reviewed data, and why the PASKWIL-2023 criteria were used despite clear deviations from international standards. Additionally, the input of patient associations should have been discussed in the HTA report.
In this preliminary relief proceedings, however, the court could not assess whether abemaciclib met the state-of-the-art. The HTA body should therefore "redo its homework" and reconsider its assessment. There was no reason to impose a penalty payment or to order the withdrawal of the report. The claimed compensation for extrajudicial costs was also rejected, but the HTA body was ordered to pay the costs of the proceedings.
Comply or explain
This legal ruling adopts a typical “comply or explain” approach, requiring the HTA body to either adhere to “standards” or provide an explanation if they choose not to comply. This approach is crucial for maintaining transparency and trust in the HTA process, helping stakeholders understand the rationale behind decisions.
But HTA bodies often diverge from international guidelines or each other for several reasons. Common reasons for divergence include uncertainties regarding clinical data, concerns about cost-effectiveness, or factors specific to the national context.
There may also be other underlying concerns that are not easy to address, such as the lack of transparency and impartiality in reports, guidelines, publications, expert opinions, and national interest.
Challenges faced by HTA bodies regarding abemaciclib
1- Concerns regarding the data
Although the Lilly’s Case implies that the Dutch are overlooking the scientific evidence for adjuvant abemaciclib, several independent international experts have also voiced concerns regarding this indication (Akhade et al., 2022; Meirson et al., 2023, Haslam et al., 2024 also covered here). Aspects such as bias in trial design, including the absence of a placebo control and not facilitating cross-over at relapse for the control group, informative censoring, lack of OS benefit, and even the potential for worse OS with adjuvant abemaciclib with longer follow-up, invasive disease-free survival not being a valid indicator for OS, treatment toxicity, over-treatment, financial toxicity, and inconsistencies with two negative trials of CDK4/6 inhibitors in the adjuvant setting. Therefore, it is important that all HTA bodies, as well as companies and regulators, take the concerns of independent experts seriously and consider how they can address them. Only in this way we can stimulate the development of treatments that truly improve patients' lives.
2- Considering the national context
Factors such as differences in healthcare systems and available healthcare budgets and resources, patient demographics and healthcare needs, cultural aspects and willingness to pay play an important role in HTA decision-making. Additionally, the comparator can vary between countries, creating differences in comparative efficacy analysis. As part of the national context, the local medical society may have a different perspective on what is considered clinically meaningful, such as the Dutch PASKWIL criteria. Medical societies that aim to raise standards should be supported and applauded.
3- Concerns regarding a lack of transparency and competing interests.
Most foreign HTA reports black out critical details concerning costs, cost-effectiveness and unpublished clinical data. Moreover, it is often not transparent how the competing interests of experts and reviewers are addressed, nor to what extent national interests play a role in decision-making. A local HTA may have to lower standards to support local industry and economic growth. For instance, the policy changed in the United Kingdom (UK) after Brexit due to concerns regarding companies leaving the country, not launching products or deprioritizing the UK market. To enhance market attractiveness, the National Institute for Health and Care Excellence (NICE) relaxed its appraisal standards and modified the thresholds for cost-effectiveness to increase the number of positive recommendations. Additionally, a commercial framework was introduced in England to facilitate access to medicines that exceed the approval threshold through complex commercial arrangements and confidential discounts.
4- Competing interests amoung medical societies, experts, KOLs and guidelines committees.
The EU Court of Justice has recently annulled a negative assessments of the EMA, because a member of an ad hoc expert group consulted by the agency had also provided consultancy services for several pharmaceutical companies, and another member was the principal investigator of a competing trial. According to the court:
“The fact that, at the end of its discussions and deliberations, that expert group expresses its opinion collegially does not remove such a defect. That collegiality is not such as to neutralise either the influence that the member in a situation of conflict of interest is in a position to exert within that group or the doubts as to the impartiality of that group which are legitimately based on the fact that that member was able to contribute to the discussions.”
In other words, the presence of a single expert with competing interests can influence the group's impartiality and raise doubts about its neutrality.
In such a case, it is not even necessary to “provide proof of specific indications of bias, such as statements or positions taken by the expert within the group. Objective impartiality is to be assessed independently of the specific conduct of the person concerned.” This is important in light of the joint EU HTA set to begin in 2025, as the HTA cannot be advised by experts who have competing interests. Accordingly, local and international guideline committees may need to revise their regulations.
Taken together, this legal case emphasizes the importance of 'comply or explain,' while also highlighting the challenges faced by a country—here, the Netherlands—willing to raise standards for assessing evidence. This decision sets a worrying precedent in drug regulation worldwide, and the reassessment of abemaciclib by the Dutch HTA body should be closely followed.
 | A guest post by
|
Great insights and coverage, thank you Sahar van Waalwilk !
This is a terrible precedent... Many 'positive' RCT's suffer shortcomings in design, execution and interpretation. The low bar set by FDA and EMA nonetheless leads to approvals of drugs lacking any real proof of benefit. Forcing a local HTA to reevaluate a carefully made negative decision of this trial (see also Meirson et al Lancet Oncol. 2023 Jun;24(6):589-593.) is just worrying. This will ultimately only harm breast cancer patients and society. I fear more cases (for access to other non-effective, interventions lacking proof) will follow...