

Dostarlimab in Mismatch Repair-Deficient, Locally Advanced Rectal Cancer: The Next Magic Bullet?

Earlier this year, the FDA Oncologic Drugs Advisory Committee (ODAC) voted in support of further clinical evaluation of dostarlimab, a novel anti-PD-1 monoclonal antibody, in patients with dMMR/MSI-H locally advanced rectal cancer.
This announcement is the latest in the ongoing development and discussion surrounding dostarlimab, which we previously commented on in light of its impressive Phase II results.
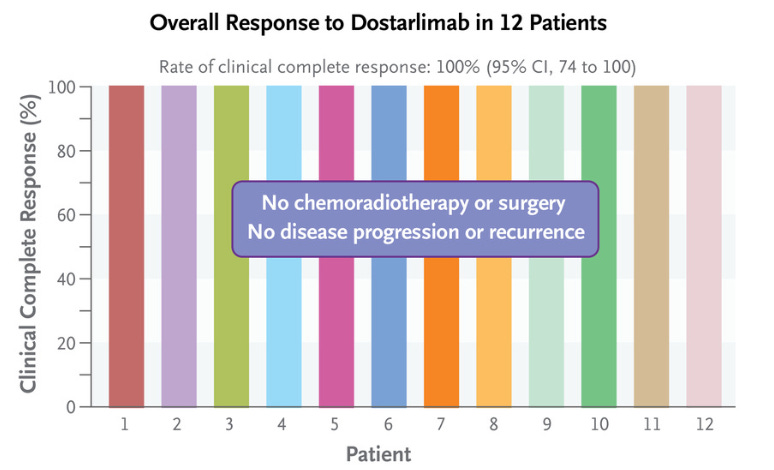
To recap, among the first 12 patients with dMMR/MSI-H locally advanced rectal cancer treated with dostarlimab, 100% achieved a clinical complete response. Furthermore, as of current reporting, there have been no occurrences of disease progression/recurrence or the need for chemoradiotherapy (CRTx) and surgery.
Many communicators have touted dostarlimab a ‘breakthrough’ with others going so far as to refer to the novel therapeutic as a ‘parachute.’ While these claims may seem exciting, they’ve also raised concerns regarding the need for further evaluation of dostarlimab with randomized controlled trials (RCT), the gold standard of evidence.
The Current Landscape
During the ODAC voting process, several members pointed out that conducting a RCT to compare dostarlimab with the current standard of care (i.e., CRTx/surgery) would be impractical due to the lack of equipoise. Instead, investigators will conduct single-arm trials measuring 12-month clinical complete response rate, which to their credit, some ODAC members expressed hesitancy about given its surrogate status (as opposed to more robust endpoints measuring survival).
However, our commentary proposed a novel trial methodology that was not discussed during these deliberations.
A Brief History
Before diving into the potential trial design, it is important to reflect on the importance of medical evidence, and the sometimes-tongue-in-cheek analogies used to dismiss its curation. RCTs are widely regarded as the ‘gold standard’ for medical evidence, thanks to their ability to minimize confounding and limit bias. RCTs are particularly useful in biomedicine, where treatment effects are often small and interventions are delivered at the individual level.
Of course, there are situations where RCTs may be less important – for example, when interventions have very large effect sizes. Here, RCTs are unnecessary due to the obvious visible benefit. Check out the schematic below for a visual representation of this concept.

An analogy often used to dismiss the need for RCTs is that of the parachute, originally coined by Smith and Pell who conducted a systematic review of RCTs of parachutes, of which there were none, subtly conveying to evidence-based medicine fanatics that randomized trials should not be conducted for medical practices with obvious benefit (i.e., or those with a 99.99% absolute risk reduction [ARR] in all-cause mortality, such as a parachute).
Though riddled with humor, it falls short in its applicability to medicine, given that medical treatments with large effect sizes are still much smaller than the effect size of parachutes. For more nuance regarding the limitations of this analogy, please read this, this, and this.
"Is it a parachute?" trial
So how do we figure out if dostarlimab is a parachute? Just as imatinib changed the landscape of cancer care when 53 out of 54 patients (98%) with chronic myeloid leukemia achieved a complete hematologic response in a phase I trial – further evaluation in RCTs was sought. We believe the process for dostarlimab should be similar.
Our proposal for evaluating dostarlimab is the following – patients would be randomized to one of three arms: dostarlimab, nivolumab, or pembrolizumab (anti-PD-1 monoclonal antibodies). To get a better idea of all of these moving parts, check out the figure.

In theory, trial enrollment on the three arms may persist as long as clinical complete responses persist without relapse. However, if a single arm exhibits signs of not being a “parachute,” such as relapse based on a pre-specified stopping rule (e.g., exceeding 5%, 10%, or 15%), that arm will no longer permit enrollment. If a second arm also exceeds the stopping rule, it will also be closed.
However, if all three arms exceed the stopping rule, then a second randomization will be initiated. Patients will be enrolled and randomized to either surgery and chemoradiotherapy, the current standard of care, or the drug that performed best in the earlier stage of the trial.
A major strength of this trial design is the continual accrual whilst within the parachute zone (i.e., the sweet spot until one of the therapies demonstrates dominance). For more information, you can read the full manuscript here.
Conclusion
In conclusion, it’s crucial that we remember the valuable lessons of the past when it comes to generating robust medical evidence: that magic bullets are few and far between, and unchecked drug development must be navigated tactfully.
The encouraging results of dostarlimab underscore the need for such an approach to ensure the best possible outcomes for patients. It's time we employ RCTs whenever possible, even if it means thinking outside the box and exploring innovative trial designs.
Abbreviations: anti-PD-1, anti-programmed death receptor-1; dMMR, mismatch-repair deficient; MSI-H, microsatellite-instability-high
 | A guest post by
|